
The New Axis of Disease: How Oral Dysbiosis Initiates Systemic Illness and What You Can Do to Save Lives, Every Day!

Professor, Department of Otolaryngology,
Division of Dentistry,
Feinberg School of Medicine,
Northwestern University
Introduction
The oral microbiome has been recently classified as a “Gateway” microbiome, giving it immense importance in total body health.(1) The placental microbiome is another gateway microbiome, that sets the immune system of the developing child, and is also extremely important. Not surprisingly it is most closely related in microbial content to the oral microbiome!(2) This scenario makes the oral microbiome most crucial for health and the most important in treatment priority. But what creates a dysbiotic oral microbiome?
Antimicrobials, both dietary and therapeutic can eliminate many protective commensals. (3-4) A sugar heavy diet supporting pathogen growth, very poor oral hygiene practices, severe dental crowding, and very importantly, mouth breathing can all negatively affect the oral microbiome. (5-6) Nutritional counseling, prebiotic and probiotic supplementation along with correction of the mouth breathing are all necessary for long term oral and systemic health. (7-8) An oral probiotic with decades of positive research is available that uses three probiotic strains to significantly improve the oral microbiome (9-11), literally changing hundreds of the other oral microbial strains! The new axis of disease consists of the following; oral dysbiosis leads to placental dysbiosis, oral dysbiosis also leads to gut dysbiosis (leaky gut) and leaky blood brain barrier. (12-14) All of this has been well accepted by the medical community because of definitive recently published research.
This recently published research has revealed the precise mechanisms used by key pathogens to suppress the host’s immune system creating a slew of systemic illnesses. (15-17) Indeed, key oral pathogens are now proven to be the determinants of the new axis of disease. With an oral dysbiosis comes an eventual gut dysbiosis leading to “leaky” gut and faulty Blood Brain Barrier. The connection has been well defined between these key pathogens and metabolic syndrome, premature birth, miscarriages, atherosclerosis, inflammatory Alzheimer’s and cancer.(18) Fortunately, we have an armamentarium of prebiotics and probiotics that can help oral healthcare professionals restore an oral eubiosis! In addition, early diagnosis and correction of mouth breathing can also benefit the oral microbiome. (19-20) Impressive new research into the many benefits of probiotics will be presented. And the surprising effect of probiotics and the microbiome affecting cancer is truly encouraging and not to be overlooked.(21)
This article will provide all the research-based information necessary to establish proper oral microbiome support in preventing dental caries, periodontal disease, metabolic syndrome, atherosclerosis, inflammatory Alzheimer’s and other associated illnesses. The latest in research proving the necessity of newer and more effective prevention protocols will be presented. In short, this is how we try to save lives, every day.

Background
How does dysbiosis occur? Unfortunately, western diet and industrialization has further influenced human health by corrupting our diet. (22) The first major change for homo sapiens happened as the hunter gatherers became horticulturists, and later even more with the Neolithic period and the advent of agriculture (grain diet).(23) Now we have the introduction of fast food and processed food, coinciding with the over-use of antibiotics, further affecting the health of humans and domestic animals.(24) Even certain anti-microbial mouth-rinses have sadly reduced our oral commensal bacteria.(25) We are truly missing many of our “old friends” when it comes to the oral and gut microbiomes. A recent study of Hadza infants demonstrated that over 23% of their gut microbiome contained bacteria that were “novel” to western nation infants.(26) Previously published research revealed that children with the diagnosis of Autism Spectrum Disease have a microbiome deficient in protective bacteria but also had pathogenic bacteria capable of affecting neurotransmitter levels theoretically necessary for “normal” neural development. (27-30)
Key pathogens
Scardovia wiggsiae is a Bacillus bacterium found extensively associated with
Severe-Early Childhood Caries. Scardovia wiggsiae and Slackia exigua have
both been reported to be involved in the early caries development.(31) Candida albicans, a fungal organism, helps with the biofilm production by increasing the extracellular polysaccharide matrix which protects Streptococcus mutans from anti-microbials and commensals such as Streptococcus oralis. (32) Lactobacilli inhibit the colonization of Candida albicans, hence decreasing the polysaccharide matrix, exposing the Streptococcus mutans to the bactericins or hydrogen peroxide of its natural competitors, other Streptococcus species. Streptococcus oralis produces hydrogen peroxide that inhibits the anaerobic Streptococcus mutans growth. (33) Indeed, Probiora probiotic, a commercially available probiotic product, contains Streptococcus oralis, uberis and rattus, and claims to inhibit several key dental pathogens. Probiotics have been reported to be an important adjunct in preventive dental care. (34-36)
Another key pathogen is Porphyromonas gingivalis. P gingivalis is an anaerobic bacterium belonging to the phylum Bacteroidetes and is a nonmotile, Gram-negative, rod-shaped, and pathogenic. Being anaerobic it is inhibited by hydrogen peroxide producing Streptococcus species such as, S. oralis and S.uberis. Porphyromonas gingivalis has been reported to be a causative agent of periodontal disease, pre-term birth, metabolic syndrome, arteriosclerosis, and inflammatory Alzheimer’s. Because P gingivalis can be considered the foremost or “keystone” initiator of periodontal disease, it is reasonable to describe it as the causal agent of Neural Arterial Gingival Simplex, a single disease with all of its associated comorbidities. (37)
P. gingivalis has also been called a “guerilla” for its notable tactics of slowly subverting the host’s defensive mechanisms. It does this in several ways:
• The host’s immunity is bypassed by the ability of P. gingivalis fimbriae to attach to hosts’ cells, like gingival epithelial cells or endothelial cells, and then invade the cell itself. Intra-cellular invasion prevents macrophages from defending the host tissue. The invaded host cell often becomes senescent, and the endopathobiont P. gingivalis remains relatively inactive until the host cell’s apoptosis.(17)
• P. gingivalis has the ability to shift genomes in different strains to specifically target different host cells, making it particularly virulent and destructive.(15)
• The epigenetic influence of P. gingivalis allows it to open the tight junctions between cells and to modulate the immune response. In addition, P. gingivalis intracellular invasion of macrophages increases the macrophages’ nitric oxide production, increasing capillary growth.(16)
In summary, P. gingivalis undermines a massive host immune response but does not normally overwhelm the host because that would effectively limit the spread of the pathogen.(17) A dead host does not help a pathogen flourish.
With the new concept of P. gingivalis infection creating a systemic single disease with multiple symptoms, it is easy to understand the processes involved. (37) The oral component houses the initial infection where the immune system is alerted and subverted, creating an inflammatory environment resulting with periodontal disease. Circulating leukocytes may carry P. gingivalis and associated lipopolysaccharides, which affect the endothelial cells of arteries, and infect the arterial walls and neural tissues, compromising the blood brain barrier. (38) This eventually diminishes the cognitive ability of the host, resulting in reduced oral hygiene and further spreading of the P. gingivalis pathogen amongst all the host’s contacts.
Prebiotics are substances that promote probiotics and possibly also inhibit pathogens. The most commonly utilized prebiotics are polyols, such as, xylitol and erythritol. Numerous studies have demonstrated the effectiveness of polyols in inhibiting cariogenic and periodontal pathogens, (39-42) Fortunately, xylitol is available in many forms making incorporation into preventatives relatively achievable. Xylitol toothpaste, mouth rinse, lollipops, candy, nasal spray, and gum is commercially available and very well accepted by patients. Studies have reported that xylitol can also prevent the transmission of cariogenic bacteria from mother to child. (43) The preventive effect, reduction in the DMFT was significantly better than the “positive” control of fluoride varnish.(44) Interestingly, xylitol is also anti-inflammatory and has proven cancer inhibitory effects, increasing the apoptosis of cancer cells and preventing angiogenesis in the tumor.(45-48) Xylitol in a nasal spray has also been documented to reduce respiratory viral load with several key viral pathogens.(49) This is in addition to the benefits of improving nasal respiration quality.(50)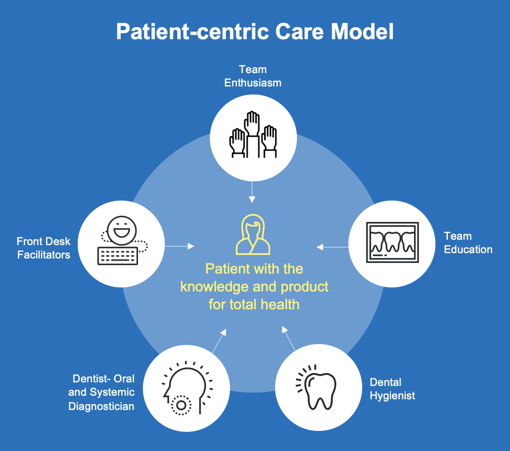
Successful implementation of a modern preventive program in dental practice must include consideration of oral and systemic health. The most important step, the very first step in implementing a modern preventive program is to totally involve the entire office staff. The whole team should be educated as to the value of “saving lives every day”. Indeed, most team members will be very enthusiastic about their new roles as total body health professionals. This requires an investment into education, as they not only need to know what to do, but why and for whom.
BRING YOUR TEAM TO AAOSH MEETINGS!
During the examinations and especially during the dental prophylaxis, the conversations should be devoted to how oral health determines gut health, and how gut health effects total systemic health. Many patients are surprised to hear the published research and are very grateful that their oral professionals are so current in their health knowledge. The frequent comment is “why am I hearing this for the first time, and why didn’t my previous dental professional tell me?” Dental hygienists have a pivotal role in this crucial period of time, reinforcing the importance of oral and systemic health. Team members can often significantly help by providing brochures, and in the case of my office, we use tear sheets with key points checked and comments circled. Having appropriate brochures and literature is very helpful for take home notes for the patients. Also, products and brochures should be prominently displayed. As the patients are walked to the reception area, key points should be reiterated and the suggested product available at the desk. Patients often will not purchase needed preventative product if it is inconvenient, so minimize the patient’s effort by always having preventative prebiotics and probiotics readily available.
The benefits are obvious to the patients and team members as oral pathology is obviously reduced in the compliant patients. The cavity rate and gingival health is always improved if the patient follows the suggested protocols. If they do come back and there is oral disease, they will most likely confess that they had inadvertently slacked off on the recommended product/protocol. In many offices, the profits from the sale of product goes into a general office fund that supports office events and education. That is a win/win for all, patients, doctors, and office team.
Conclusion
The best defense against oral and systemic disease is a healthy oral microbiome. Essential for the health of the oral microbiome, the Oral Gateway microbiome, is the significant presence of beneficial bacteria that inhibit the key pathogens. The only clinically available preventative that re-establishes the healthy oral microbiome would be an effective oral probiotic product. ProBiora is a commercially available product that contains three very important probiotic bacteria that inhibits the key pathogenic bacteria and maintains the healthy oral microbiome for total oral and systemic health. 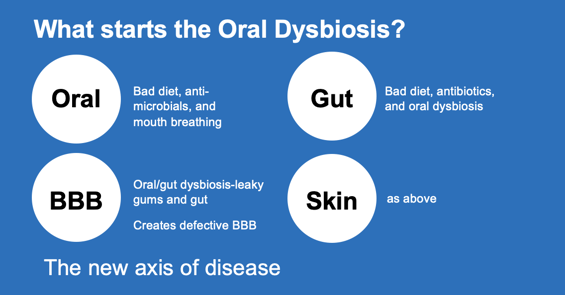
Resources
View the sample ProBiora script pad tear sheet that is available for hygienists to write out to their patients by clicking here.

Scan above or visit www.ProBioraHealth.com/dental to learn more and order ProBiora probiotics for the mouth today.
References
1. Nobel Assembly June 1-2nd., 2017-The microbiome and its programming of body systems. No 64.
2. Aagaard, Kjersti et al. “The placenta harbors a unique microbiome.” Science translational medicine vol. 6,237 (2014): 237ra65. doi:10.1126/scitranslmed.3008599
3. Marques TM, Cryan JF, Shanahan F, Fitzgerald GF, Ross RP, et al. Gut microbiota modulation and implications for host health: dietary strategies to influence the gut-brain axis (2014) Innov Food Sci Emerg Technol 22: 239-47. https://doi.org/10.1016/j.ifset.2013.10.016
4. Walsh CJ, Guinane CM, OToole PW and Cotter PD. Beneficial modulation of the gut microbiota (2014) FEBS Lett 588: 4120-4130. https://doi.org/10.1016/j.febslet.2014.03.035
5. Okada H, Kuhn C, Feillet H and Bach JF. The hygiene hypothesis for autoimmune and allergic diseases: an update (2010) Clin Exp Immunol 160: 1-9. https://doi.org/10.1111/j.1365-2249.2010.04139.x
6. Thomas S, Izard J, Walsh E, Batich K, Chongsathidkiet P, et al. The Host Microbiome Regulates and Maintains Human Health: A Primer and Perspective for Non-Microbiologists (2017) Cancer Res 77: 1783-1812. https://doi.org/10.1158/0008-5472.CAN-16-2929
7. Swartwout B and Luo XM. Implications of Probiotics on the Maternal-Neonatal Interface: Gut Microbiota, Immunomodulation, and Autoimmunity (2018) Front Immunol 9: 2840. https://doi.org/10.3389/fimmu.2018.02840
8. Tsai YL, Lin TL, Chang CJ, Wu TR, Lai WF, et al. Probiotics, prebiotics and amelioration of diseases (2019) J biomed sci 26: 3. https://doi.org/10.1186/s12929-018-0493-6
9. Singh RK, Chang HW, Yan D, Lee KM, Ucmak D, et al. Influence of diet on the gut microbiome and implications for human health (2017) J Transl Med 15: 73 https://doi.org/10.1186/s12967-017-1175-y
10. Hillman JD, Socransky SS (1989) The theory and application of bacterial interference to oral diseases. In New Biotechnology in Oral Research. ed. Myers HM (Basel: S Karger) 1-17.
11. Zahradnik RT, Magnusson I, Walker C, McDonell E, Hillman CH (2009) Preliminary assessment of safety and effectiveness in humans of ProBiora3, a probiotic mouthwash. J Applied Micro 107(2): 682-690.
12. Hajishengallis G, Darveau RP and Curtis MA. The keystone-pathogen hypothesis (2012) Nat Rev Microbiol 10: 717-725. https://dx.doi.org/10.1038%2Fnrmicro2873
13. Hajishengallis G. Porphyromonas gingivalis-host interactions: open war or intelligent guerilla tactics? (2009) Microbes infect 11: 637-645. https://doi.org/10.1016/j.micinf.2009.03.009
14. Dominy SS, Lynch C, Ermini F, Benedyk M, Marczyk A, et al. Porphyromonas gingivalis in Alzheimers disease brains: Evidence for disease causation and treatment with small-molecule inhibitors (2019) Sci adv 5: eaau3333. https://doi.org/10.1126/sciadv.aau3333
15. Tribble GD, Kerr J E, and Wang BY. Genetic diversity in the oral pathogen Porphyromonas gingivalis: molecular mechanisms and biological consequences (2013) Future microbial 8: 607-620. https://doi.org/10.2217/fmb.13.30
16. Guo W, Wang P, Liu ZH, and Ye P. Analysis of differential expression of tight junction proteins in cultured oral epithelial cells altered by Porphyromonas gingivalis, Porphyromonas gingivalis lipopolysaccharide, and extracellular adenosine triphosphate (2018) Int J oral sci 10: e8. https://doi.org/10.1038/ijos.2017.51
17. Hajishengallis G and Lamont RJ. Breaking bad: manipulation of the host response by Porphyromonas gingivalis (2014) Eur J Immunol, 44: 328-338. https://doi.org/10.1002/eji.201344202
18. Jin, L. J., Lamster, I. B., Greenspan, J. S., Pitts, N. B., Scully, C., & Warnakulasuriya, S. (2016). Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral diseases, 22(7), 609–619. https://doi.org/10.1111/odi.12428
19. Zamarron, C., García Paz, V., & Riveiro, A. (2008). Obstructive sleep apnea syndrome is a systemic disease. Current evidence. European journal of internal medicine, 19(6), 390–398. https://doi.org/10.1016/j.ejim.2007.12.006
20. Fan, C., Guo, L., Gu, H., Huo, Y., & Lin, H. (2020). Alterations in Oral-Nasal-Pharyngeal Microbiota and Salivary Proteins in Mouth-Breathing Children. Frontiers in microbiology, 11, 575550. https://doi.org/10.3389/fmicb.2020.575550
21. Gopalakrishnan, V., Helmink, B. A., Spencer, C. N., Reuben, A., & Wargo, J. A. (2018). The Influence of the Gut Microbiome on Cancer, Immunity, and Cancer Immunotherapy. Cancer cell, 33(4), 570–580. https://doi.org/10.1016/j.ccell.2018.03.015
22. Malesza, I. J., Malesza, M., Walkowiak, J., Mussin, N., Walkowiak, D., Aringazina, R., Bartkowiak-Wieczorek, J., & Mądry, E. (2021). High-Fat, Western-Style Diet, Systemic Inflammation, and Gut Microbiota: A Narrative Review. Cells, 10(11), 3164. https://doi.org/10.3390/cells10113164
23. Stefano, G. B., Fine, R., & Kream, R. M. (2018). Microbiome and Health: Ramifications of Intelligent Deception. Medical science monitor : international medical journal of experimental and clinical research, 24, 2060–2062. https://doi.org/10.12659/msm.910248
24. Grech, A., Collins, C. E., Holmes, A., Lal, R., Duncanson, K., Taylor, R., & Gordon, A. (2021). Maternal exposures and the infant gut microbiome: a systematic review with meta-analysis. Gut microbes, 13(1), 1–30. https://doi.org/10.1080/19490976.2021.1897210
25. Kapil, V., Haydar, S. M., Pearl, V., Lundberg, J. O., Weitzberg, E., & Ahluwalia, A. (2013). Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free radical biology & medicine, 55, 93–100. https://doi.org/10.1016/j.freeradbiomed.2012.11.013
26. Olm, M. R., Dahan, D., Carter, M. M., Merrill, B. D., Yu, F. B., Jain, S., Meng, X., Tripathi, S., Wastyk, H., Neff, N., Holmes, S., Sonnenburg, E. D., Jha, A. R., & Sonnenburg, J. L. (2022). Robust variation in infant gut microbiome assembly across a spectrum of lifestyles. Science (New York, N.Y.), 376(6598), 1220–1223. https://doi.org/10.1126/science.abj2972
27. MacFabe DF, Cain NE, Boon F, Ossenkopp KP and Cain DP. Effects of the enteric bacterial metabolic product propionic acid on object-directed behavior, social behavior, cognition, and neuroinflammation in adolescent rats: Relevance to autism spectrum disorder (2011) Behav Brain Res 217: 47-54. https://doi.org/10.1016/j.bbr.2010.10.005
28. Rose S, Bennuri SC, Davis JE, Wynne R, Slattery JC, et al. Butyrate enhances mitochondrial function during oxidative stress in cell lines from boys with autism (2018) Translational Psychiatry 8: 42. https://doi.org/10.1038/s41398-017-0089-z
29. Wikoff WR, Anfora AT, Liu J, Schultz PG, Lesley SA, et al. Metabolomics analysis reveals large effects of gut microflora on mammalian blood metabolites (2009) Proceedings of the National Academy of Sciences of the United States of America, USA 106: 3698-3703. https://doi.org/10.1073/pnas.0812874106
30. Argou-Cardozo I and Zeidán-Chuliá F. Clostridium Bacteria and Autism Spectrum Conditions: A Systematic Review and Hypothetical Contribution of Environmental Glyphosate Levels (2018) Med Sci (Basel) 6: 29. https://doi.org/10.3390/medsci6020029
31. Fakhruddin, K. S., Ngo, H. C., & Samaranayake, L. P. (2019). Cariogenic microbiome and microbiota of the early primary dentition: A contemporary overview. Oral diseases, 25(4), 982–995. https://doi.org/10.1111/odi.12932
32. Xiao, J., Huang, X., Alkhers, N., Alzamil, H., Alzoubi, S., Wu, T. T., Castillo, D. A., Campbell, F., Davis, J., Herzog, K., Billings, R., Kopycka-Kedzierawski, D. T., Hajishengallis, E., & Koo, H. (2018). Candida albicans and Early Childhood Caries: A Systematic Review and Meta-Analysis. Caries research, 52(1-2), 102–112. https://doi.org/10.1159/000481833
33. Hillman, J. D., Socransky, S. S., & Shivers, M. (1985). The relationships between streptococcal species and periodontopathic bacteria in human dental plaque. Archives of oral biology, 30(11-12), 791–795. https://doi.org/10.1016/0003-9969(85)90133-5
34. Cannon M (2011) A Review of Probiotic Therapy in Preventive Dental Practice. Probiotics Antimicrob Proteins 3(2): 63-67.
35. Cannon M, Trent B, Vorachek A, Kramer S, Esterly R (2013) Effectiveness of CRT at measuring the salivary level of bacteria in caries prone children with probiotic therapy. J Clin Pediatr Dent 38(1): 55-60.
36. Cannon M (2011) Clinical Application of Probiotic Therapy. Inside Dentistry 7(6): 112-113.
37. Cannon ML and Peldyak JN. The prevention and treatment of neural arterial gingival simplex (2019) Dental Res Manag 3: 32-37
38. Xu, T., Dong, Q., Luo, Y., Liu, Y., Gao, L., Pan, Y., & Zhang, D. (2021). Porphyromonas gingivalis infection promotes mitochondrial dysfunction through Drp1-dependent mitochondrial fission in endothelial cells. International journal of oral science, 13(1), 28. https://doi.org/10.1038/s41368-021-00134-4
39. Janakiram C, Deepan Kumar CV and Joseph J. Xylitol in preventing dental caries: a systematic review and meta-analyses (2017) J Nat Sci Biol Med 8: 16-21. https://doi.org/10.4103/0976-9668.198344
40. Badet C, Furiga A and Thébaud N.Effect of xylitol on an in vitro model of oral biofilm (2008) Oral Health Prev Dent 6: 337-341.
41. Janus MM, Volgenant CMC, Brandt BW, Buijs MJ, Keijser BJF, et al. Effect of erythritol on microbial ecology of in vitro gingivitis biofilms (2017)J Oral Microbiol 9: 1. https://doi.org/10.1080/20002297.2017.1337477
42. Söderling E, Hietala and Lenkkeri AM. Xylitol and erythritol decrease adherence of polysaccharide-producing oral streptococci (2010) Curr Microbiol 60: 22-29. https://doi.org/10.1007/s00284-009-9496-6
43. Söderling E, Isokangas P, Pienihäkkinen K and Tenovuo J. Influence of maternal xylitol consumption on acquisition of mutans streptococci by infants (2000) J Dent Res 79: 882-887. https://doi.org/10.1177/00220345000790031601
44. Isokangas, P., Söderling, E., Pienihäkkinen, K., & Alanen, P. (2000). Occurrence of dental decay in children after maternal consumption of xylitol chewing gum, a follow-up from 0 to 5 years of age. Journal of dental research, 79(11), 1885–1889. https://doi.org/10.1177/00220345000790111201Xylitol cancer
45. Tomonobu, N., Komalasari, N., Sumardika, I. W., Jiang, F., Chen, Y., Yamamoto, K. I., Kinoshita, R., Murata, H., Inoue, Y., & Sakaguchi, M. (2020). Xylitol acts as an anticancer monosaccharide to induce selective cancer death via regulation of the glutathione level. Chemico-biological interactions, 324, 109085. https://doi.org/10.1016/j.cbi.2020.109085
46. Park, E., Park, M. H., Na, H. S., & Chung, J. (2015). Xylitol induces cell death in lung cancer A549 cells by autophagy. Biotechnology letters, 37(5), 983–990. https://doi.org/10.1007/s10529-014-1757-1
47. Sahasakul, Y., Angkhasirisap, W., Lam-Ubol, A., Aursalung, A., Sano, D., Takada, K., & Trachootham, D. (2022). Partial Substitution of Glucose with Xylitol Prolongs Survival and Suppresses Cell Proliferation and Glycolysis of Mice Bearing Orthotopic Xenograft of Oral Cancer. Nutrients, 14(10), 2023. https://doi.org/10.3390/nu14102023
48.
